

Let me start with something you won’t find in any medical textbook: The first time I heard someone talk about perimenopause, I thought it was a rare condition—like an allergy or something that would skip me, surely. Years later, after waking up sweaty at 2AM and feeling like my memory had holes, I realized I was just woefully unprepared, like so many women. As you'll see, perimenopause and menopause remain shrouded in misconception, mystery, and even a hint of denial in our culture—including science itself! This post combines science, stories, and a touch of rebellion to decode what’s really happening, why it matters for vitality and mental health, and what practical steps you can actually take—before, during, and after the ‘zone of chaos.’
Redefining Menopause: More Than the Absence of a Period?
When you hear the word “menopause,” what comes to mind? For many, it’s the classic medical definition: one year after your last menstrual period. But is this really the best way to understand such a complex transition? Let’s unravel why this period-based milestone may not capture the full story of menopause symptoms, hormonal changes, and the true biological journey your body is experiencing.
The Traditional Definition: Why It Misses the Mark
For decades, menopause has been defined by a simple calendar rule: if you haven’t had a period for twelve months, you’re officially menopausal. As one expert put it,
“The medical definition of menopause, which I have a huge problem with, is one year after the final menstrual period.”
But what if you don’t have periods to count? Maybe you’ve had a hysterectomy, use an IUD, had an endometrial ablation, or live with PCOS. In these cases, tracking menstruation changes doesn’t work. Even clinicians find it challenging to diagnose menopause in women who don’t fit the textbook pattern. This approach leaves many women without clear answers, even as they experience classic menopause symptoms like hot flashes, sleep problems, and mood swings.
The “One Day” Problem: Beyond the Calendar
Here’s another wrinkle: menopause, by definition, is just one day—exactly one year after your last period. But the reality is far more complicated. Menopause is not just a date; it’s the permanent end of ovarian function. It’s a process, not a single event. Your hormones don’t just switch off overnight. Instead, they shift and decline over time, leading to a range of hormonal changes that affect everything from your mood to your bones.
Ovarian Aging: The Real Biological Clock
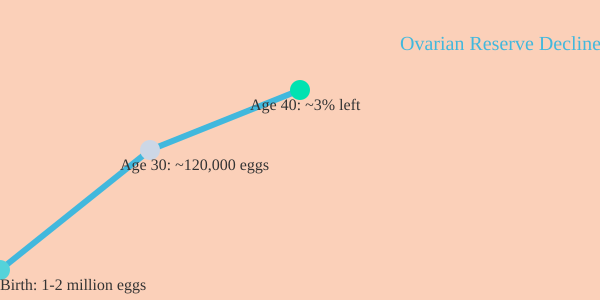
So what’s really happening inside your body? Unlike men, who produce new sperm throughout life, you’re born with all the eggs you’ll ever have—about 1 to 2 million. By age 30, you’re down to roughly 120,000 eggs, or about 10% of your original supply. By age 40, you have just 3% left. As one clinician notes,
“By the time we're forty, we're down to three percent of our egg supply.”
And it’s not just about quantity. Egg quality declines as well, making conception harder and hormonal fluctuations more pronounced. This gradual depletion of the ovarian reserve is what truly drives the transition into menopause—not just the absence of a period.
Hormonal Changes: Estradiol, Progesterone, and Testosterone
As your egg supply dwindles, your ovaries produce less estradiol and progesterone. Research shows estradiol levels drop to less than 1% of what they were in your reproductive years. Progesterone, which has calming and sleep-promoting effects, also plummets. Testosterone declines too, but only to about 50% of its peak, since your body can make it elsewhere.
- Estradiol levels: Drop to less than 1% of reproductive peak
- Progesterone effects: Decrease, leading to more anxiety and sleep issues
- Testosterone: Falls to about half of youthful levels
These hormonal changes explain why menopause symptoms vary so much. Some women breeze through with few issues; others struggle with hot flashes, mood swings, brain fog, and more. The experience is deeply personal and shaped by your unique biology.
Should We Rethink Menopause?
Given all this, is it time to redefine menopause? Many experts think so. Instead of focusing on menstruation changes, perhaps we should talk about “ovarian senescence” or “ovarian failure”—terms that reflect the underlying biology. After all, the average age for menopause in the U.S. is 51 to 52, but the normal range is 45 to 55. And for many women, the classic definition simply doesn’t fit.
In the end, menopause is about much more than the absence of a period. It’s a profound biological shift—one that deserves a definition as nuanced and dynamic as the women who experience it.
Welcome to the Zone of Chaos: Perimenopause Demystified
If you’ve ever wondered why your body suddenly feels unpredictable in your 40s or early 50s, you’re not alone. Perimenopause, often called the “zone of chaos” by experts, is a transition phase that can start as early as seven to ten years before your final menstrual period. For many, that means perimenopause symptoms begin in the mid-40s, though the timing can vary widely from person to person. In fact, research shows there’s significant variation in how women experience this stage—some may breeze through with barely a blip, while others find themselves navigating a storm of hormonal changes and menstruation changes that seem to defy logic.
What makes perimenopause so confusing? It’s all about your hormones. In your reproductive years, your menstrual cycle is like a well-rehearsed orchestra—estrogen, progesterone, and brain hormones like LH and FSH rise and fall in a predictable monthly rhythm. But as you approach perimenopause, that harmony starts to unravel. Your ovaries become less responsive to the usual hormonal cues, especially to FSH (follicle-stimulating hormone) and LH (luteinizing hormone). The brain, sensing that estradiol levels are dropping, tries to compensate by sending out stronger and more frequent pulses of FSH. Sometimes, the ovaries respond; sometimes, they don’t. The result? Hormonal chaos.
You might notice your periods changing—sometimes they come closer together, sometimes they’re further apart. They might become heavier, lighter, or just plain unpredictable. Estradiol levels, a key form of estrogen, can spike higher than you ever saw in your younger years, only to plunge to new lows the next month. This volatility is why experts describe perimenopause as “literal hormonal chaos.” As one clinician put it:
“We call it in our world, the zone of chaos. So it is literal hormonal chaos.”
These hormonal changes in perimenopause don’t just affect your cycle. You may experience a wide range of perimenopause symptoms, including:
- Hot flashes (affecting 35%–75% of women, sometimes lasting years beyond menopause)
- Mood changes—depression, anxiety, irritability, or sudden crying spells
- Sleep disturbances, often linked to night sweats or anxiety
- Vaginal dryness, which can cause discomfort or pain during sex
- Brain fog, memory lapses, and trouble focusing (reported by about 60% of women)
- Changes in menstruation—heavier or lighter periods, or cycles that are closer together or farther apart
What’s especially challenging is that there’s no single blood test that can confirm you’re in perimenopause. Because estradiol and FSH levels can swing wildly—even within the same month—lab results are often misleading. Diagnosis is usually based on your symptoms and by ruling out other possible causes. This can be frustrating, especially when you’re seeking answers and clarity.
Adding to the confusion, many doctors themselves are only now receiving comprehensive training about perimenopause. For decades, medical education focused more on menopause itself, leaving a gap in understanding the years leading up to it. As a result, you might find that you know more about your own symptoms than your healthcare provider does. This lack of awareness is common—studies indicate that many women don’t even realize they’re in perimenopause until symptoms become disruptive.
The unpredictability of perimenopause can feel overwhelming, but understanding the science behind these changes can help you navigate this phase with more confidence and less fear. Here’s a quick look at the key facts:
| Key Aspect | Details |
|---|---|
| Perimenopause Onset | ~7-10 years before menopause (often mid-40s) |
| Hormonal Changes | FSH and estradiol levels surge and drop unpredictably |
| Cycle Changes | Menstruation becomes irregular—heavier, lighter, closer or farther apart |
| Diagnosis | No reliable lab test; based on symptoms and ruling out other causes |
As you move through this “zone of chaos,” remember: you’re not alone, and your experience is valid—no matter how unpredictable it feels. The more you know about perimenopause symptoms, hormonal changes, and menstruation changes, the better equipped you’ll be to advocate for your health and well-being.
Mental Health in Menopause: Far More Than Mood Swings
When you think about menopause, you might picture hot flashes or changes in your period. But what’s often overlooked is how deeply menopause mental health is affected. In fact, for many women, the first signs of perimenopause aren’t physical at all—they’re mental. Mood changes, anxiety symptoms, depression, and even sudden irritability can appear long before the classic physical symptoms. If you’ve ever found yourself forgetting appointments, struggling to focus, or feeling unlike yourself, you’re not alone. These are common experiences, and science is finally catching up to explain why.
The Brain: A Hormone Powerhouse
Your brain is flooded with hormone receptors—estrogen, progesterone, and testosterone all play a role in how your mind works. These hormones don’t just affect your body; they’re crucial for brain chemistry. Research shows that as hormone levels become chaotic during perimenopause and menopause, neurotransmitters like serotonin, dopamine, and norepinephrine are thrown off balance. This can lead to a wide range of menopause mental health symptoms, from mood swings to full-blown depression perimenopause.
Mood Changes and Mental Health: The Hidden Symptoms
It’s not just about feeling “a little off.” Studies indicate that mood changes, anxiety, depression, and crying spells are common during this transition. In fact, about 1 in 4 women will experience a major depressive episode during menopause. What’s even more surprising is that these mental health symptoms often outpace the physical ones. You might notice anxiety symptoms or irritability before you ever miss a period or have a hot flash.
Brain Fog and Memory Problems: More Than Just Forgetfulness
Ever walk into a room and forget why you’re there? Or lose track of a conversation mid-sentence? This “brain fog” is a real and under-reported complaint. Research shows that up to 60% of menopausal women experience brain fog, memory problems, and trouble focusing. It’s not just about aging—it’s about how your hormones are interacting with your brain’s executive function. These lapses can be frustrating and even scary, but they are a normal part of the menopause journey for many.
What the Data Tells Us
| Symptom or Change | Prevalence/Increase |
|---|---|
| Mental health disorders during menopause transition | 40% increase |
| SSRI (antidepressant) use | Doubles during perimenopause/menopause |
| Brain fog, memory, and focus problems | ~60% of menopausal women affected |
"We have at least a Forty percent increase of mental health disorders and SSRI use doubles across the menopause transition."
Hormone Therapy: A New Hope for Depression Perimenopause
For years, antidepressants like SSRIs were the go-to solution for menopause mental health issues. But new research is shifting that thinking. Studies now suggest that hormone therapy during perimenopause can actually help prevent new cases of depression—and in some cases, it may outperform traditional antidepressants. Neuroscientists are beginning to recognize that giving estrogen to women developing depression in perimenopause can lead to better outcomes than SSRIs alone. This is a big shift, and it’s changing how doctors approach menopause-related mood changes.
Why This Matters: Normalizing the Experience
It’s easy to feel isolated or even ashamed when your mind doesn’t work the way it used to. I remember the anxiety that hit me after I forgot an important appointment—my brain just felt different. It was unsettling. But here’s the thing: you’re not alone, and you’re not “losing it.” These changes are a direct result of the complex dance between your hormones and your brain. Every woman deserves to have this experience normalized and understood.
What You Can Do
- Talk openly with your healthcare provider about mood changes, brain fog, or memory problems.
- Track your symptoms—mental and physical—to spot patterns.
- Ask about hormone therapy if you’re struggling with depression perimenopause or anxiety symptoms.
- Remember: seeking help is a sign of strength, not weakness.
Menopause mental health is far more than mood swings. It’s a complex, science-backed reality that deserves attention, compassion, and curiosity.
Symptoms, Surprises, and Stats: What Really Happens During Perimenopause and Menopause?
If you’re approaching your 40s or 50s, you might be bracing yourself for the rollercoaster of perimenopause and menopause symptoms. Maybe you’ve heard about hot flashes, mood changes, or sleep problems from friends or family. But here’s the real surprise: what you experience may look nothing like what your mother or sister went through. In fact, research shows that menopause symptoms can vary dramatically from woman to woman—there’s truly no “one size fits all.”
Common Menopause and Perimenopause Symptoms: More Than Just Hot Flashes
Let’s start with the basics. The most talked-about menopause symptom is the hot flash. Studies indicate that hot flashes affect 35%–75% of perimenopausal and menopausal women, and they can last anywhere from a few minutes to several years past your last period. But that’s just the tip of the iceberg.
- Sleep problems: Difficulty falling or staying asleep is common, often triggered by night sweats, anxiety, or even urinary problems.
- Vaginal dryness: As estrogen drops, vaginal tissues thin and dry out, leading to discomfort and sometimes pain during sex.
- Mood changes: Irritability, anxiety, and even major depression episodes can strike—about 1 in 4 women experience significant depression during this time.
- Cognitive changes: “Brain fog,” trouble focusing, and memory lapses affect roughly 60% of women in menopause.
- Sexual desire decline: Shifts in hormones can lower libido, making intimacy feel different or less appealing.
- Urinary problems: Increased urgency, frequency, or even incontinence can crop up due to changes in pelvic tissues.
Beyond the Physical: Emotional and Cognitive Shifts
Menopause symptoms aren’t just physical. You might notice your executive function—things like planning, multitasking, or remembering appointments—feels off. This is because your brain is rich in hormone receptors, especially for estrogen and progesterone. When these hormones fluctuate, neurotransmitters like serotonin and dopamine get thrown off balance, which can lead to mood instability or even new-onset depression. In fact, research shows that mental health disorders increase by at least 40% during the menopause transition, and SSRI use doubles.
“Hot flashes affect 35%–75% of perimenopausal and menopausal women, lasting from minutes to years beyond menopause.”
Surprising Variability: Your Experience Is Unique
One of the most important things to remember is that not everyone has every symptom. Some women breeze through menopause with barely a hot flash, while others struggle with a mix of physical and emotional challenges. Even within families, experiences can be wildly different. I’ll never forget the jaw-dropping moment when I compared my own menopause symptoms to my mother’s—her journey was nothing like mine. This variability is normal, and it’s why listening to your own body is so important.
When Symptoms Last and When Conditions Worsen
Hot flashes can be fleeting or stick around for years. Sleep problems might come and go, or persist long after your periods stop. And for some, conditions like fibroids or endometriosis can actually worsen during perimenopause, thanks to hormonal ups and downs. Lower estrogen levels also accelerate your risk for cardiometabolic diseases post-menopause, so it’s not just about comfort—it’s about long-term health, too.
Menopause Symptoms by the Numbers
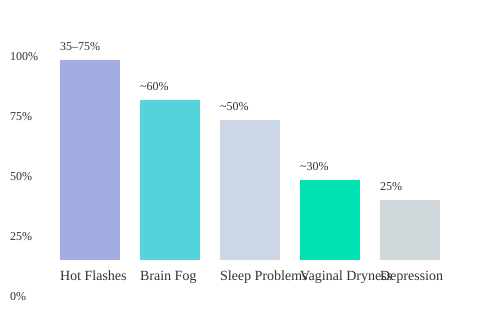
This chart highlights just how common—and variable—menopause symptoms can be. Hot flashes top the list, but brain fog, sleep problems, vaginal dryness, and depression are all significant players. Remember, your experience is unique, and what’s “normal” for you may not be for someone else.
The Research Gap: Why Science Has Largely Ignored Perimenopause (And Why That Matters)
If you’ve ever felt like perimenopause is a mystery, you’re not alone. For decades, women’s health science has overlooked this crucial stage, leaving many with more questions than answers. The numbers are striking: search PubMed, the world’s largest biomedical database, and you’ll find about 1.1 million articles on pregnancy. Type in “menopause,” and that drops to 97,000. Now, try “perimenopause”—you’ll see only around 6,400 results. As one expert put it:
“Type in the word pregnancy, one point one million articles come up. Type in the word menopause, it’s down to ninety seven thousand.”
This stark disparity in menopause research funding and attention isn’t just a quirk of academic interest. It shapes what doctors know, how symptoms are treated, and even how you might understand your own body. Historically, most medical research—especially in animal models—focused on males. Until recently, even mouse studies, which form the backbone of early biomedical research, rarely included female subjects. The National Institutes of Health (NIH) only began requiring the inclusion of female animals as a biological variable in grant-funded research in the past few years. This shift is forcing the research community to play catch-up, but the gap is still wide.
Why does this matter? When research overlooks perimenopause, it leads to poor understanding and, often, misdiagnosis. Many women don’t even realize they’re entering perimenopause until symptoms become disruptive. Hot flashes, mood swings, brain fog, and sleep problems can all appear suddenly, yet few are prepared for them. Studies show that awareness of perimenopause is low, with many women unaware until symptoms begin. This lack of perimenopause awareness means symptoms are often dismissed or misunderstood, both by patients and healthcare providers.
The consequences go beyond discomfort. Without robust women’s health science focused on perimenopause, there’s a delay in developing effective therapies and a risk of under-treating or mismanaging symptoms. For example, hormonal fluctuations during perimenopause can trigger depression, anxiety, and irritability. About 1 in 4 women will experience a major depressive episode during this time, but many are left without targeted support. Vaginal dryness, sexual pain, and changes in menstruation are also common, yet often minimized or attributed to other causes.
Another overlooked insight: aging later—experiencing menopause at an older age—correlates with better cardiometabolic health. Research shows that women who reach menopause later tend to have a reduced risk of heart disease and other metabolic conditions. Yet, this knowledge isn’t widely integrated into routine care or public health messaging. Most women aren’t told that the timing of menopause can impact long-term health, and few resources exist to help prolong ovarian function or manage this transition proactively.
So, why has perimenopause been ignored for so long? Partly, it’s the legacy of a research system that didn’t see female biology as a priority. For years, the assumption was that studying men (or male animals) would be “good enough.” Only recently has the tide begun to turn, with new guidelines and a growing push for menopause research funding. But the field is still catching up, and the effects of this historic neglect are felt every day in clinics and homes.
If you’re wondering what can be done, it starts with awareness. The more we talk about perimenopause, the more likely it is to attract research dollars and attention. And as funding grows, so does the potential for better care, earlier diagnosis, and new therapies that address the real needs of women in midlife. In the meantime, staying curious and informed is one of the best tools you have—because science is finally starting to listen, but it’s up to all of us to keep the conversation going.
Hormone Replacement Therapy, Nutrition & Lifestyle: Myths, Evidence, and Everyday Tools
When you first hear about hormone replacement therapy (HRT) for menopause symptoms, it’s easy to get lost in the noise. There’s controversy, confusion, and a lot of outdated advice. Why? Because HRT isn’t a one-size-fits-all solution. The timing, benefits, and risks of hormone therapy depend on your unique health profile, family history, and even the stage of perimenopause or menopause you’re in.
Why Is Hormone Replacement Therapy So Controversial?
Let’s start with the basics. HRT usually means supplementing estrogen, progesterone, and sometimes testosterone. But the science shows that when you start HRT matters almost as much as whether you start. If you begin hormone therapy early in perimenopause, the benefits can outweigh the risks for many women. However, starting later or with certain health conditions can change the risk profile entirely.
Doctor Marie Claire Haver emphasizes that “the specific timing in which hormone therapy is initiated plays a key role in whether or not the hormone therapy is beneficial for women or not.” This is why you’ll hear so many conflicting stories—what worked for your friend or your mother may not be right for you.
What Do We Really Know (and Not Know) About HRT?
- Estrogen: Often prescribed to reduce hot flashes, night sweats, and vaginal dryness. Research shows hot flashes affect 35%–75% of women in perimenopause and menopause, sometimes lasting years.
- Progesterone: Not just for balancing estrogen, but also for its anti-anxiety and sleep-promoting effects. Many women find progesterone helps with sleep problems, which are common during menopause.
- Testosterone: Less commonly discussed, but can play a role in libido and energy. The evidence is still emerging, and not all women benefit from testosterone therapy.
It’s important to note that not all women experience menopause symptoms the same way. Mood changes, brain fog, and even depression can show up, often unexpectedly. In fact, about 1 in 4 women will experience a major depression episode during menopause, and up to 60% report memory or focus problems.
HRT vs. SSRIs: New Evidence for Depression in Perimenopause
For years, doctors have prescribed SSRIs (antidepressants) for mood changes and depression perimenopause. But new research suggests that hormone therapy may be more effective for some women. As one study puts it:
'Women who are given hormone therapy in their perimenopause have a lower incidence of new onset depression.'
This doesn’t mean SSRIs have no place, but it does highlight the importance of personalized care. If you’re struggling with mood swings or depression, talk to your doctor about whether HRT could be a better fit for you.
Lifestyle Tools: Nutrition, Sleep, and Smart Self-Care
Hormone therapy isn’t the only answer. Nutrition and lifestyle changes can make a big difference in how you experience menopause symptoms. Simple tweaks—like increasing protein, adding resistance training, and focusing on anti-inflammatory foods—can help manage weight gain, bone loss, and inflammation.
Sleep problems are another major challenge. Hot flashes, anxiety, and even urinary changes can disrupt your rest. Research shows that optimizing your sleep environment can help. Smart mattress covers like EightSleep allow you to control temperature throughout the night, supporting the natural drop in body temperature needed for deep sleep. Even small changes, like keeping your room cool or using a fan, can make a difference.
Everyday Tools & Science-Oriented Brands
- AeroPress: For many, a good cup of coffee is a daily ritual. AeroPress offers a simple, clean way to brew coffee, supporting your morning routine without bitterness or hassle.
- EightSleep: Smart mattress covers that help you track and optimize sleep, crucial for managing menopause symptoms.
- BetterHelp: Online therapy can be a lifeline for emotional support, especially during times of hormonal change.
Conversations That Matter
Don’t underestimate the power of talking with your doctor—and your mother. Family history can reveal patterns and risks that generic pamphlets never mention. Ask about menopause symptoms, depression perimenopause, and any history of hormone replacement therapy in your family. This context can help you and your healthcare provider make the best choices for your health.
Ultimately, navigating perimenopause and menopause is about curiosity, courage, and a willingness to try science-backed tools. Whether it’s hormone replacement therapy, nutrition menopause management, or simply better sleep, you have more options than ever before.
Real Talk and Rebel Advice: How to Prepare at Every Stage
If you’re reading this, you’re already ahead of the curve. The truth is, many women don’t even know what perimenopause is until the symptoms hit—and by then, it can feel like you’re scrambling to catch up. Research shows that early menopause education awareness is empowering, yet cultural silence and medical myths often keep women in the dark. So, what does real preparation look like? It’s not just about stocking up on supplements or reading pamphlets in your doctor’s office. It’s about starting honest conversations, building a support network, and learning to advocate for yourself at every stage.
Let’s begin with the basics: talk early, talk often. If you can, ask your mother, your aunt, or any woman you trust about their experience. You might be surprised by what you learn—sometimes, the most valuable menopause education comes from real stories, not textbooks. Your OB-GYN is a good resource, but remember, not all clinicians are experts in menopause symptoms or perimenopause symptoms. If your concerns are brushed aside or you’re told “it’s just stress,” that’s a red flag. Trust your instincts. Self-advocacy is the most effective health tool most women never use. If you feel unheard, seek a second opinion or find a provider who takes your symptoms seriously.
Community support is another crucial piece of the puzzle. There’s power in sharing your story, even the parts that feel embarrassing or strange. Maybe you’re struggling with hot flashes that leave you drenched at work, or you’ve noticed your moods swinging wildly from one day to the next. You’re not alone. Studies indicate that hot flashes affect up to 75% of women during perimenopause and menopause, and mood changes—like anxiety, irritability, or even episodes of depression—are common. When you open up, you invite others to do the same, and suddenly the silence starts to break. This tradition of wisdom-sharing is as old as time, and it’s one of the best ways to prepare for what’s ahead.
Here’s a thought: what if menopause is nature’s punk rock phase? It’s disruptive, yes, but maybe it’s also a chance to rewrite your rhythms, set new boundaries, and rethink self-care. The unpredictability of perimenopause symptoms—brain fog, sleep problems, changes in your cycle—can feel chaotic. But it’s also a reminder that you get to decide how to respond. Maybe you’ll start journaling your symptoms, keeping track of what helps and what doesn’t. Maybe you’ll build a “health circle”—a few trusted friends, a therapist, or an online community—to lean on when things get tough.
Preparation isn’t just medical; it’s emotional and social, too. Therapy, for example, can be as important as exercise when it comes to navigating these changes. As one expert put it,
'I now consider doing therapy as important as getting regular exercise.'Therapy isn’t just for crisis moments. It’s a space to process shifting identities, changing relationships, and the new boundaries you may need to set. Quality therapy, especially with someone who understands the unique challenges of menopause, can help you direct your focus toward what really matters.
Finally, don’t underestimate the power of practical tools. Cooling sheets, comfortable clothing, supplements (after consulting with your provider), or even simple breathing exercises can make a real difference. Keep a journal, not just for symptoms but for wins—big or small. Celebrate the days you feel strong, and give yourself grace on the days you don’t.
In the end, preparation is about more than managing menopause symptoms. It’s about claiming agency, breaking the silence, and finding community support in unexpected places. Whether you’re just starting to notice changes or you’re deep in the thick of it, remember: you’re not alone, and you have more power than you think. Stay curious, stay courageous, and keep talking—because real talk is the first step to real change.
TL;DR: Perimenopause and menopause are chaotic, poorly understood, and often overlooked phases of life that affect not just bodies but minds, relationships, and futures. With science, proactive care, and open conversation, these transitions can be navigated for maximum vitality. Know the signs, trust your instincts, and demand better care—it's time to end the silence and rewrite the story.
Post a Comment